Conference talk
Are reimbursement pathways ready for licensed psychedelic therapies in Europe?

Slide transcript
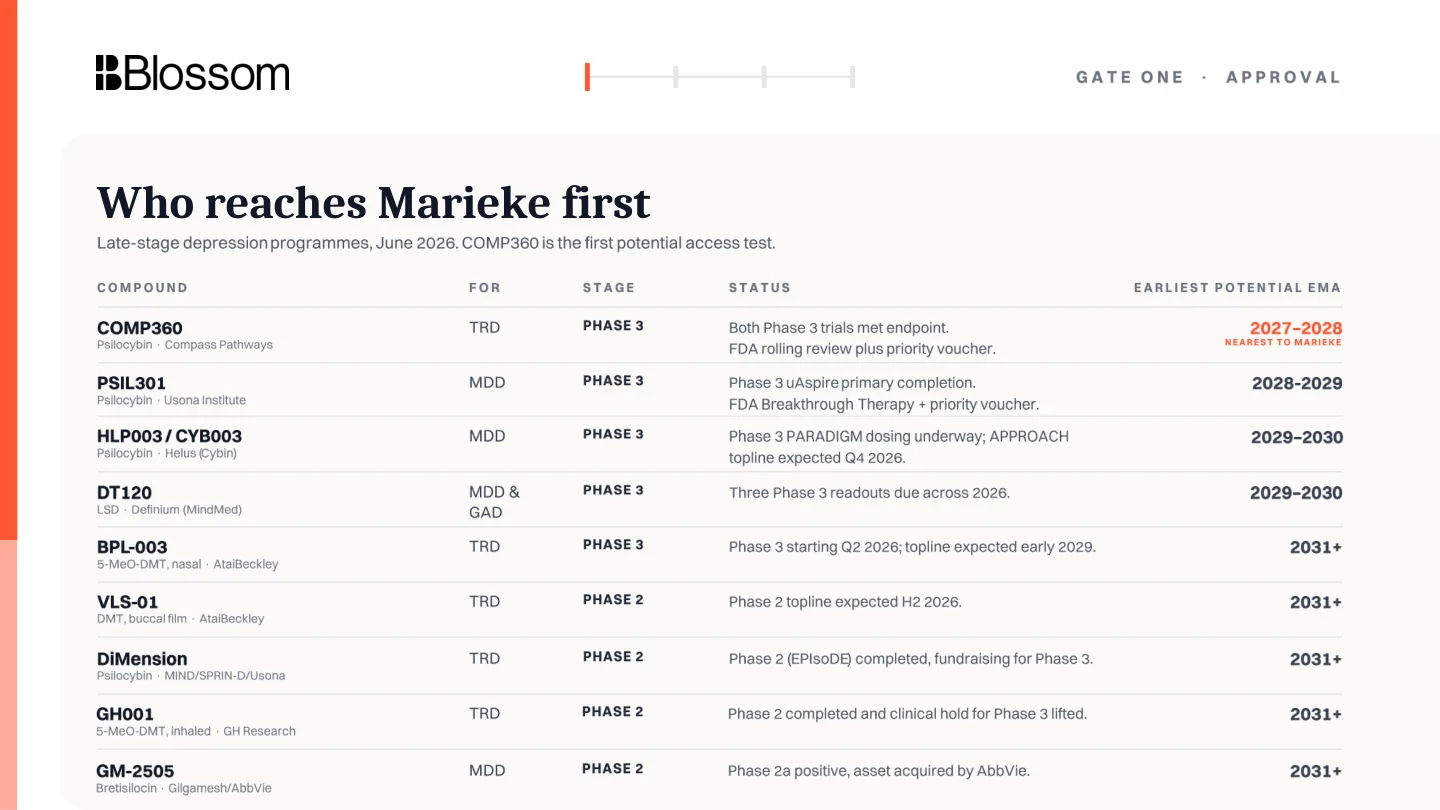
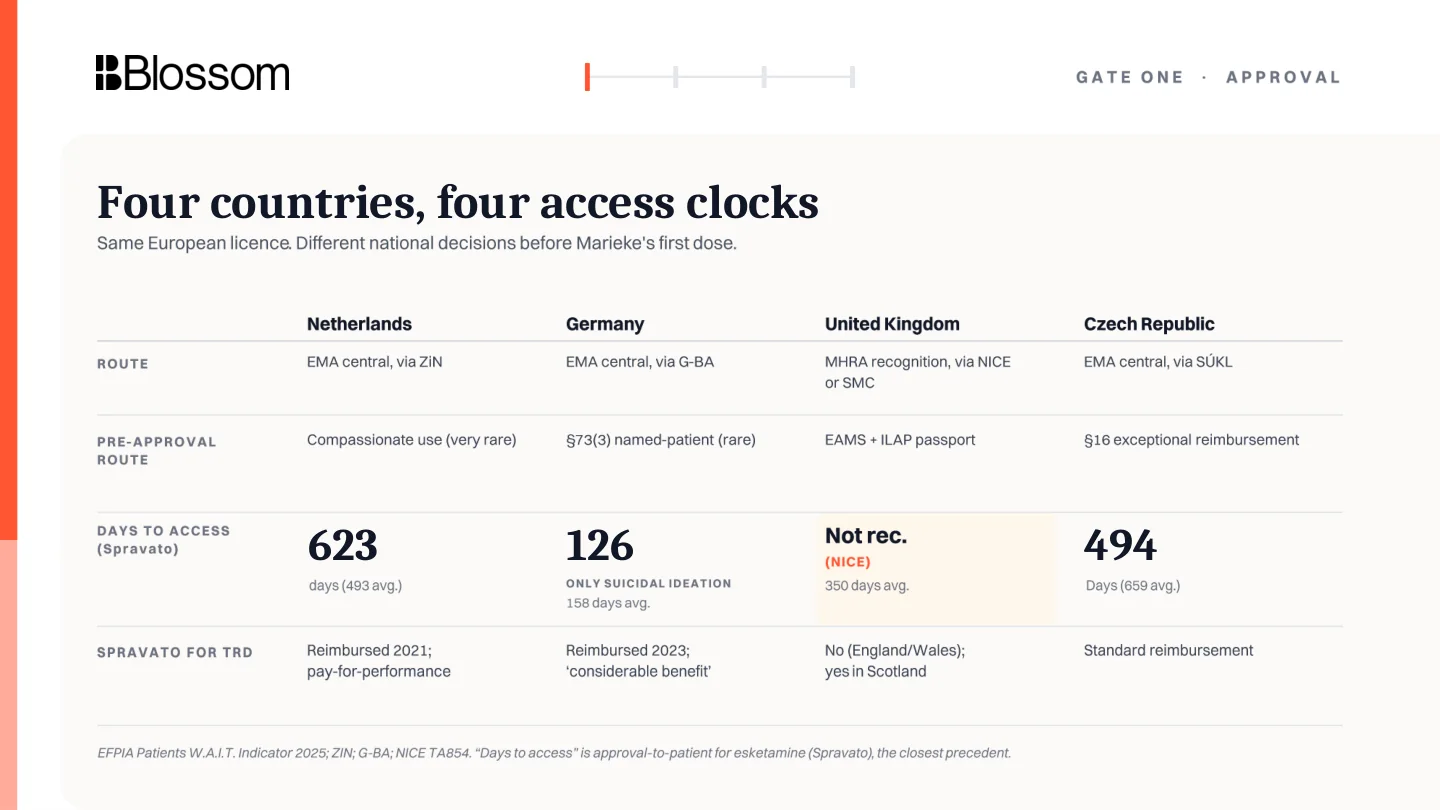
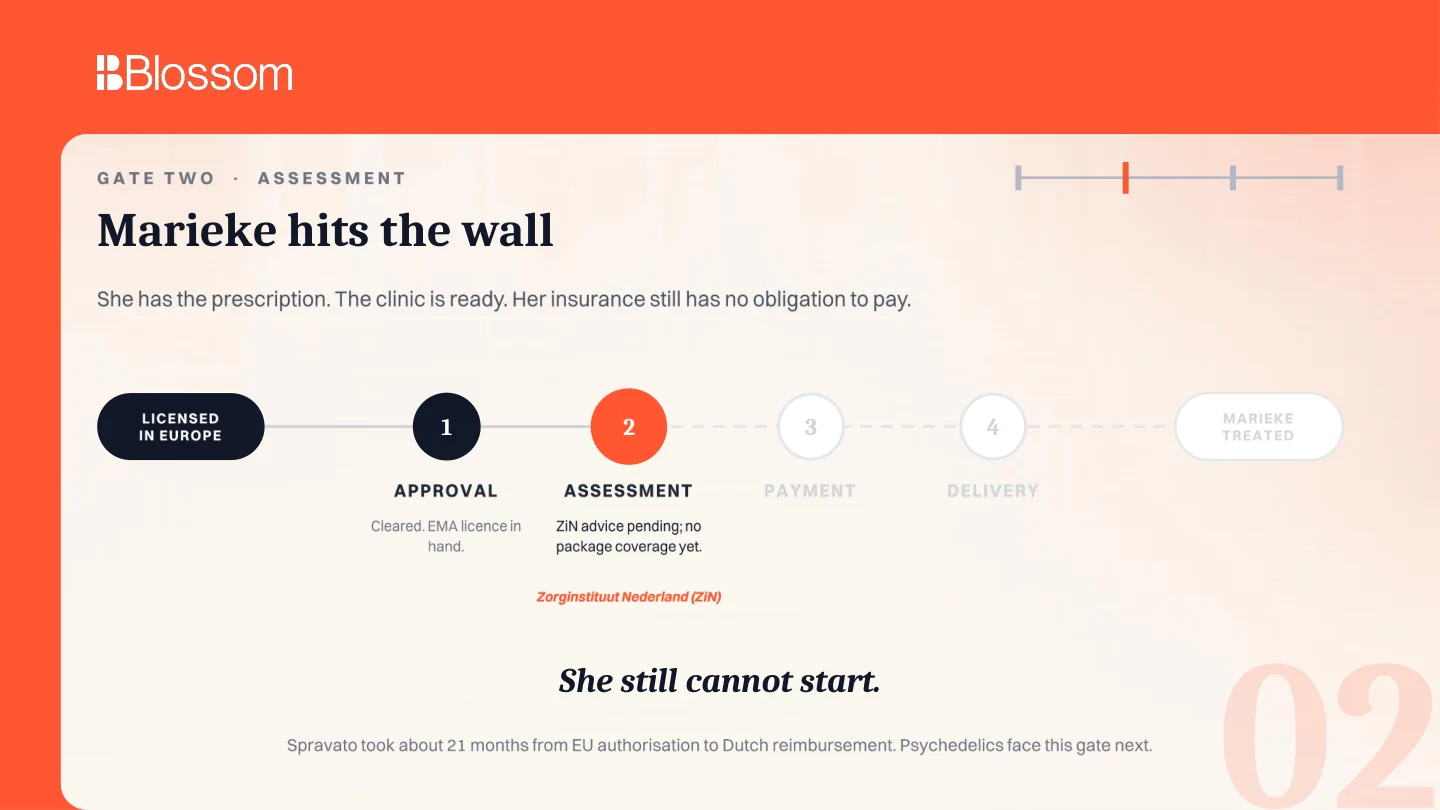
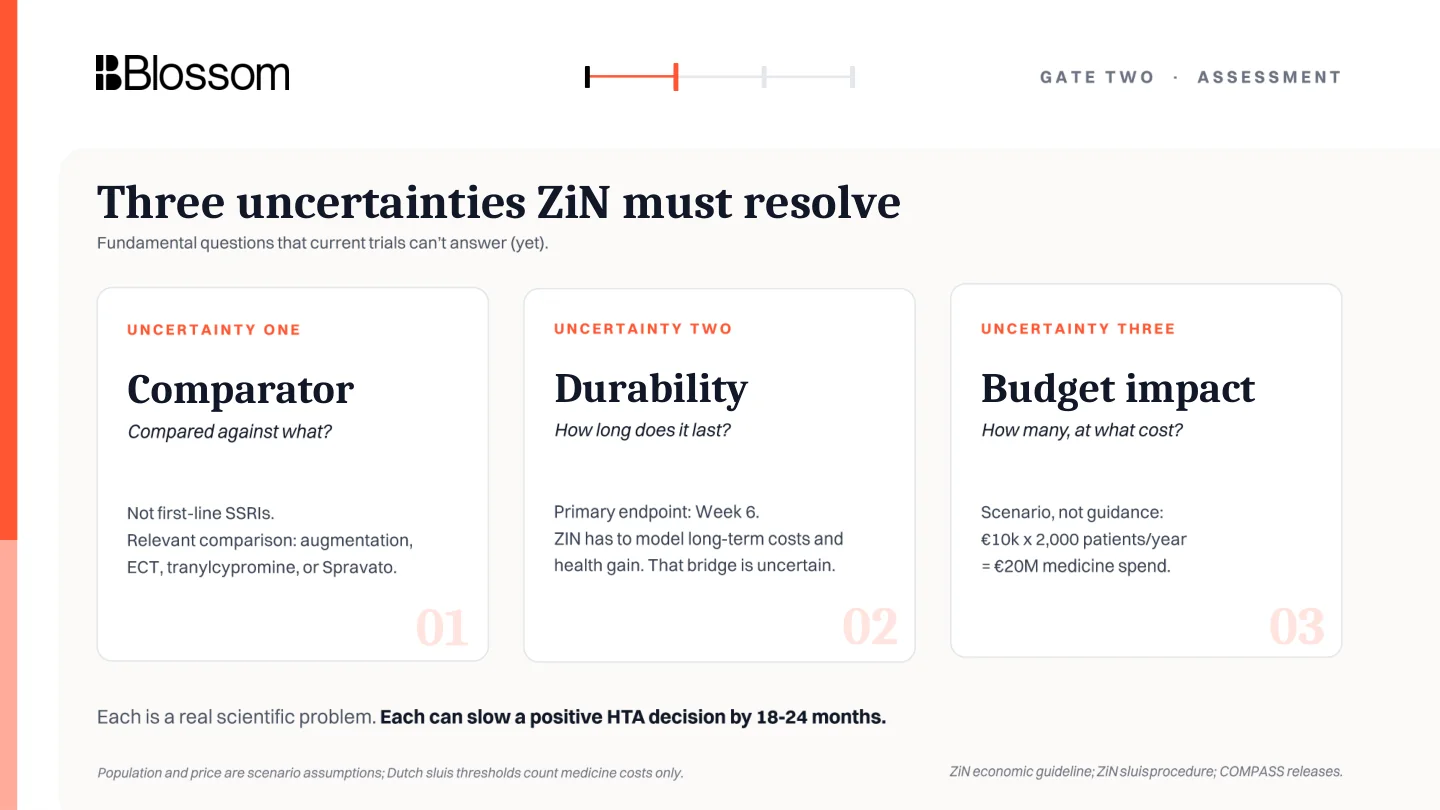
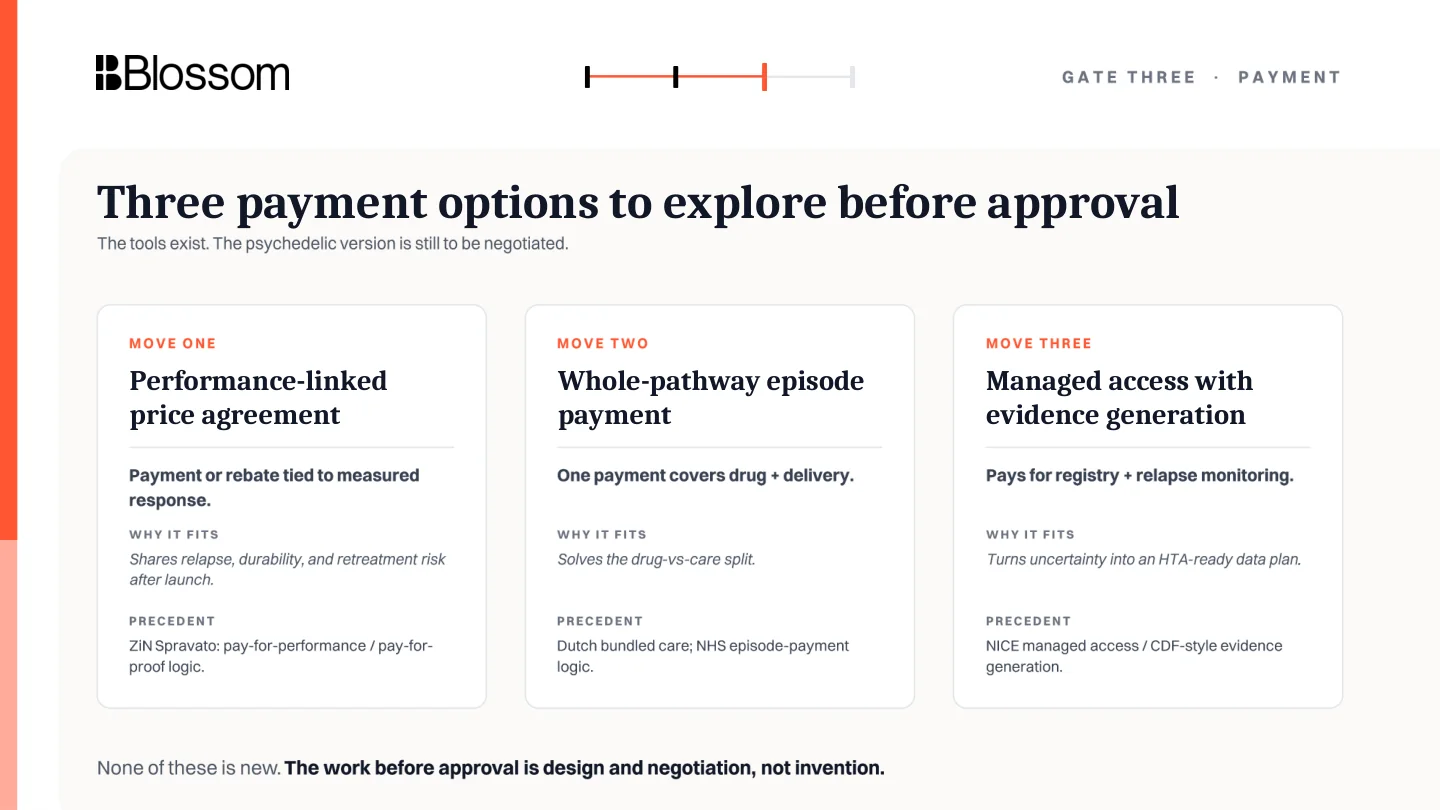
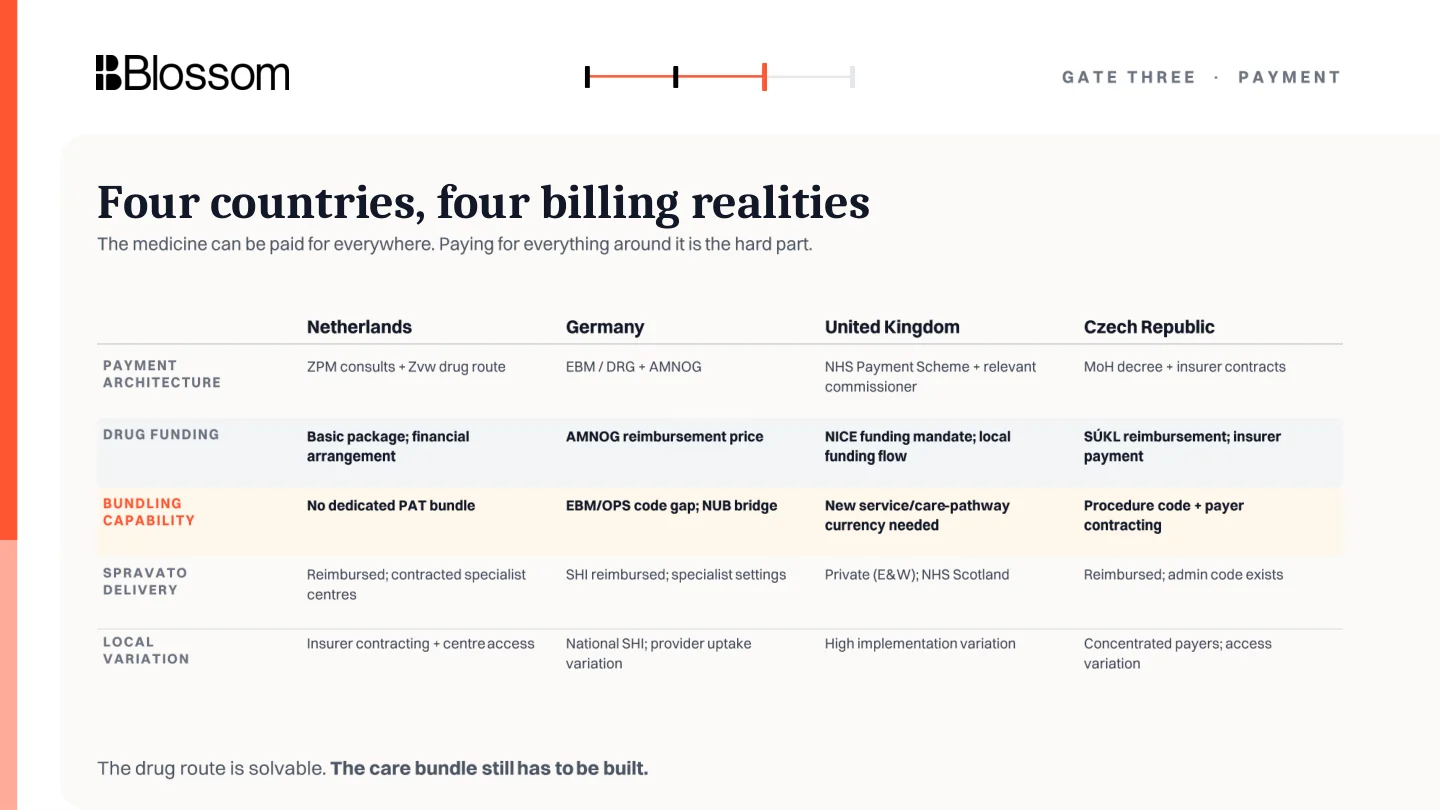
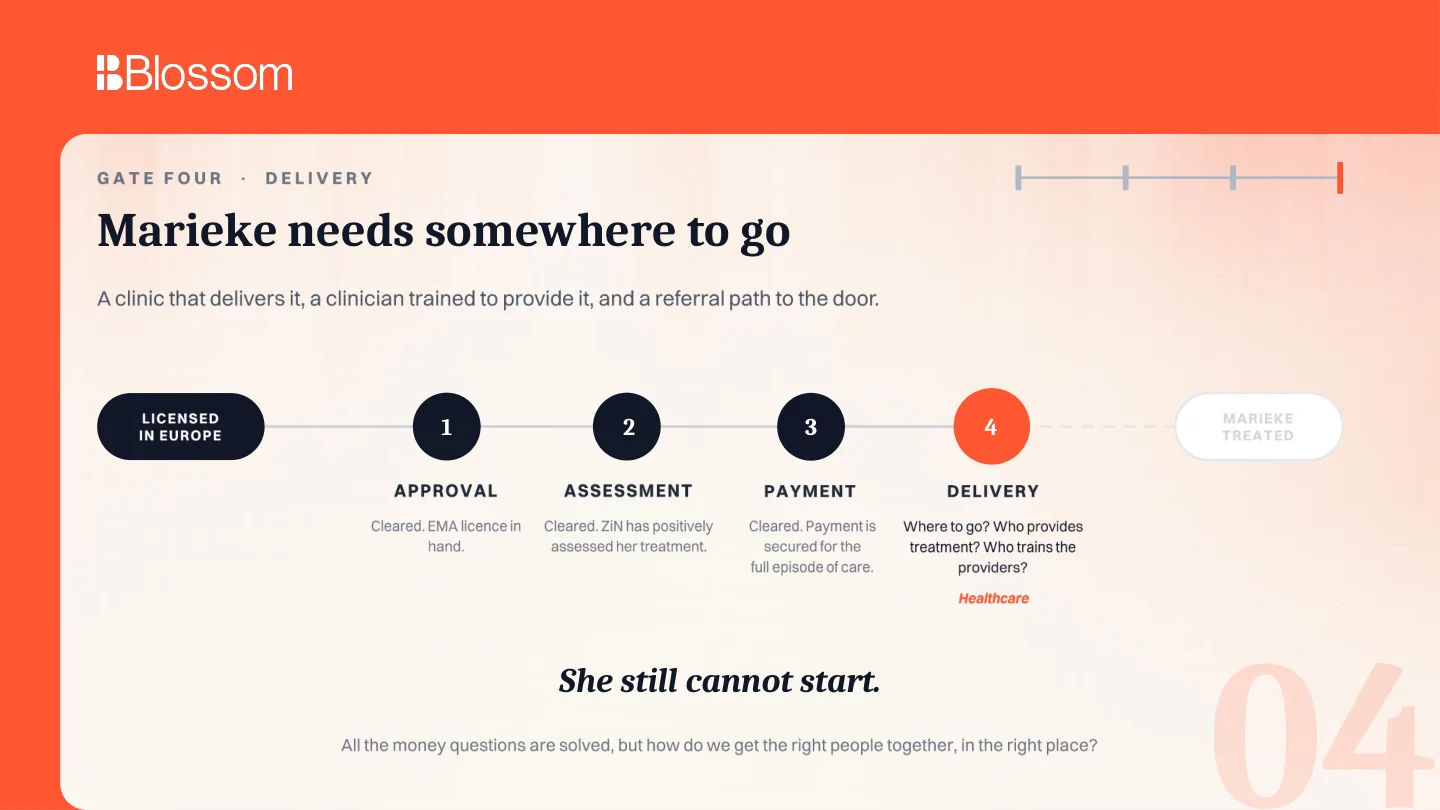
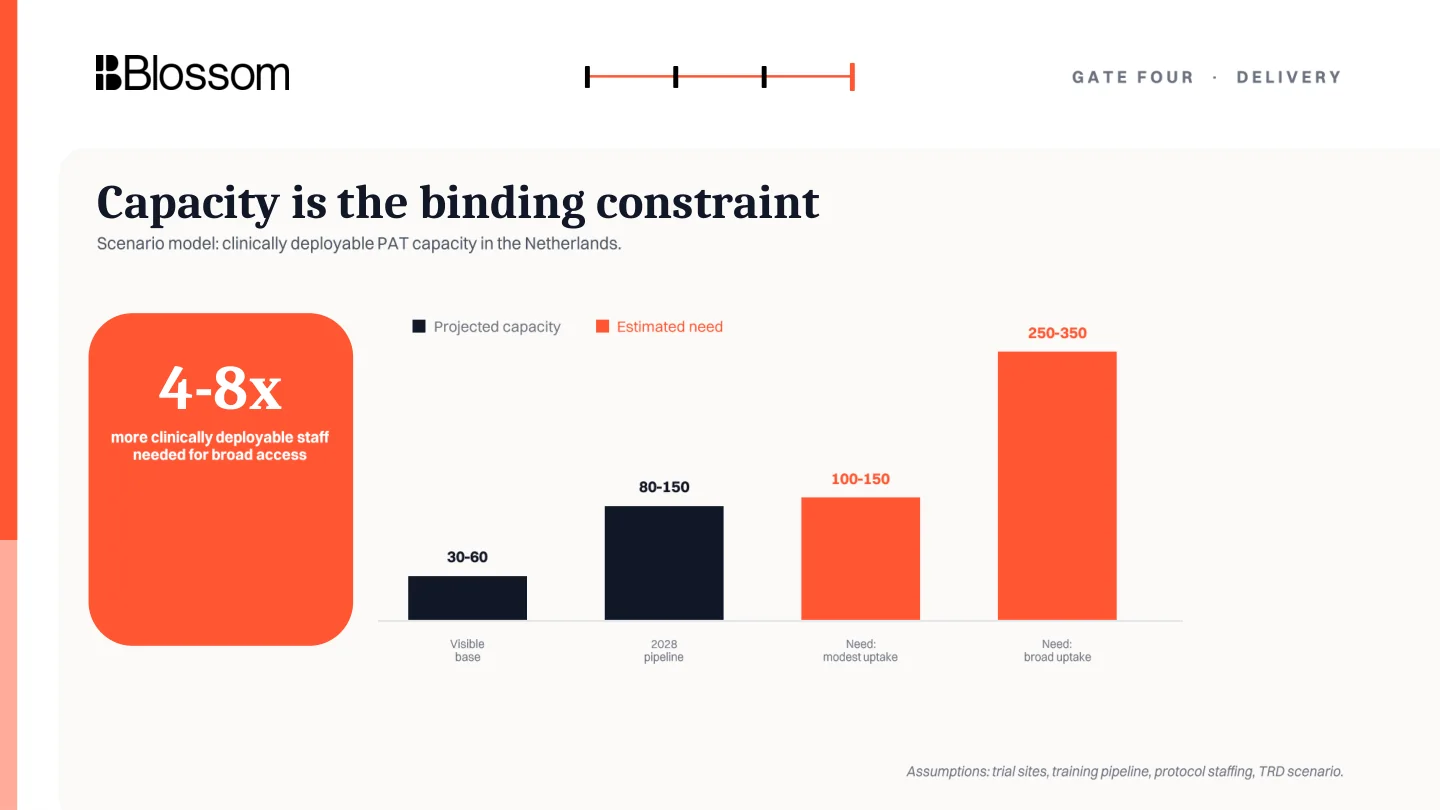
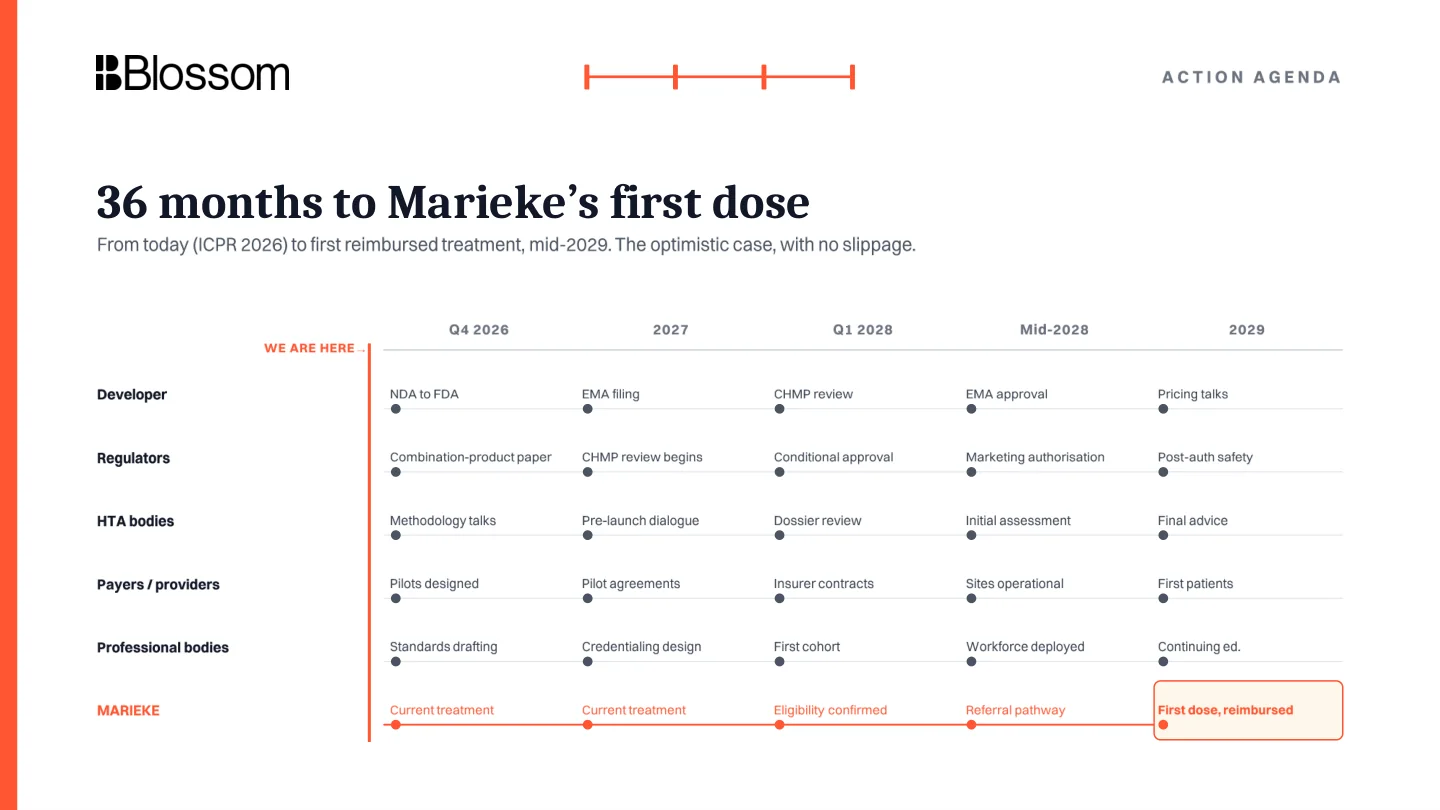
This talk asks a practical question: are European reimbursement pathways ready for licensed psychedelic therapies?
I am Floris Wolswijk, founder of Blossom, a consultant with Delphi, and a volunteer with the OPEN Foundation. The talk sits inside Blossom's broader Road to Access work on how promising treatments actually reach patients.